Dealing with Superior Canal Dehiscence Syndrome and my MFC Surgery at UCLA
Welcome to my Journey
Dealing with Superior Canal Dehiscence Syndrome and my MFC Surgery at UCLA
Welcome to my Journey

Welcome, my name is Vittorio and this website contains the story of my journey dealing with SCDS (Superior Canal Dehiscence Syndrome) from diagnosis to successful surgery at the UCLA Ronald Regan Hospital. This rare, debilitating and very strange syndrome was discovered relatively recently 1999 by Dr. Lloyd Minor at Johns Hopkins Universi
Welcome, my name is Vittorio and this website contains the story of my journey dealing with SCDS (Superior Canal Dehiscence Syndrome) from diagnosis to successful surgery at the UCLA Ronald Regan Hospital. This rare, debilitating and very strange syndrome was discovered relatively recently 1999 by Dr. Lloyd Minor at Johns Hopkins University and there in not much literature, studies and information about it. As a patient, I found it especially hard to understand the process of undergoing surgery to alleviate the symptoms and I believe that that lack of information makes many patients postpone or avoid surgery forcing them to live with a horrible quality of life.
This is why I decided to share my story here with a video journal of my surgery experience at the Ronald Regan's UCLA Hospital with Dr. Yang and Dr. Gopen. I trust this will help others as they ponders the pros and cons of surgery.
Spoiler alert: my story as of one week after surgery has a happy ending as I resolved most of my symptoms and I am quickly getting back to a normal life.
And of course, THE INFORMATION ON THIS PAGE SHOULD NOT BE CONSIDERED MEDICAL ADVICE. I am sharing my experience as a data point. Every person and every situation is different, therefore I encourage you to do your own research, listen to your doctors and so that you can make the best decision for yourself. I wish you the best possible outcome.
Scroll down to the bottom of this page for the video chronicle of the surgery or check out my YouTube Channel

In this section I will try to explain SCDS in layman terms, the way I understand it. Please refer to the links and videos in this page for more detailed and accurate description of this syndrome, or check the video library I put together here.
Superior Canal Dehiscence Syndrome (SCDS) is a condition characterized by hearing and balance issues resulting from a thinning of the temporal bone covering the superior semicircular canal of the vestibular system. As illustrated in the accompanying images, the inner ear typically consists of three circular canals responsible for both hearing and balance. In SCDS, a third hole (dehiscence) forms in the upper semicircular canal, allowing internal body sounds to be heard. This leads to the following symptoms:
It's important to note that not everyone experiences all symptoms simultaneously. For instance, in my case, I primarily dealt with autophony and some degree of brain fog.
The exact causes of SCDS are not fully understood, but there is a consensus on several factors. Approximately 2.5% of individuals have a thinner bone covering their upper semicircular canal in the inner ear, predisposing them to SCDS. Over time, the constant expansion and contraction of the brain, combined with movements such as bouncing during physical activity, can cause the canal to develop a dehiscence, allowing internal body sounds to interfere with hearing and balance. In some cases, symptoms may arise without a complete hole forming, as a result of a very thin bone structure. Additionally, head trauma and exposure to noisy environments are highly correlated with the onset of SCDS; many patients report experiencing a concussion or working in professions involving loud noise before symptom onset. It's important to note that symptoms may not immediately follow head trauma; for instance, in my case, symptoms emerged several years after a concussion. Some individuals may have lived with the syndrome their entire lives, and many go undiagnosed for years due to limited awareness of the condition. While symptoms may not necessarily worsen over time, there is insufficient data on this, and they often fluctuate based on factors such as noise levels, overall health, and intracranial pressure.
To diagnose SCDC, doctors use a combination of these tools:
The challenge is finding an ENT doctor and a radiologist who even know about this syndrome. Most people get mis-diagnosed as simple tinnitus, or vertigo or even dismissed as if their symptoms were imaginary.
There's no denying it—SCDS symptoms are distressing and overwhelming. Constantly hearing internal body noises can feel like a never-ending nightmare, not to mention the accompanying balance issues. Individuals experiencing these symptoms often spiral into depression, struggle with sleep, withdraw from social activities to avoid exacerbating noises, and may even stop working altogether. It's truly debilitating.
My heart goes out to those who remain undiagnosed and must endure these symptoms.
Personally, I also experienced a very dark period for the first 4-5 months after receiving the initial diagnosis (more details below), but I was able to regain stability through sheer determination, meditation, exercise, and the unwavering support of friends and family.
There are two main support group on Facebook (as on February 2018).
The original one managed by Ann and started in 2010. You can find it by clicking here.
There is a another support group on Facebook with thousands of members managed by Pamela and Karen. It is the best place to find people facing similar symptoms, asking questions, getting help and support. You have to have been diagnosed with SCDS to join. Here is the link.

The primary treatment for SCDS is surgery, although not everyone is a suitable candidate and finding a surgeon skilled in the procedure can be challenging. However, for those who undergo surgery, the success rate is typically high. As of 2018, there are two main types of surgeries for SCDS:
1. Middle Fossa Cranial (MFC) Surgery: This procedure involves two surgeons—a neurosurgeon to access the skull and lift the brain, and an ENT surgeon to address the dehiscence by either plugging or resurfacing it.
2. Transmastoid Superior Canal Occlusion (TM) Surgery: This surgery can be performed solely by an ENT surgeon.
Some surgeons also perform the "Minimally Invasive Approach via Transcanal Oval and Round Window Reinforcement." However, this approach lacks sufficient success data to be considered mainstream and effective. In this discussion, I will focus on MFC (the procedure I underwent) and TM surgery.
With MFC, the surgeon opens up a hole on the side of the skull (middle fossa), lift the base on the brain to get access to the inner ear, then either plugs or resurfaces the area where the dehiscent is or both depending on the surgeon and the patient situation. Once the hole is sealed, the repair is pretty much done and in 85-90% of cases the auditory symptoms are gone. Patients with balance problems may still struggle with balance but they can start vestibular rehabilitation few weeks after surgery, which seem to help may.
There is still very little history about this syndrome and the surgery repairs to draw firm conclusions between plugging or resurfacing the hole. Here are the main pros and cons:
The team lead by Dr. Yang and Dr. Gopen at UCLA has developed an innovative technique to further minimize the hole in the skulls that results in a less invasive procedure. This is the surgery ended up choosing with hole resurfacing using bone wax. More on why later in the details of my journey.
With the Transmastoid surgery approach, a hole is drilled in the temporal bone on the side of the ear to reach the superior canal, which then gets either plugged or cut and plugged. At the highest level, it seems that this approach is more appropriate for patients that have both auditory (autophony) as well as vestibular problems. The surgery, pretty much disables the balance organ in that ear and overtime the brain learn to rely on the other ear for balance.
Everybody should do their own research and talk to their medical team about what option is the best based on symptoms, state of the art technology and surgeon's skills. Here is an article that compares the outcome of the two techniques.
According to this published article, it looks like the MFC approach has a higher level of success compared to TM.
The Massachusetts Eye and Ear Hospital seems to perform both type of surgeries. you can find out more here.
Here is a success story for the SCDS TM Surgery.
The number of surgeons that perform this surgery is ever increasing but my research in 2017 led me to zero in on these three centers that seems to have the most experience with SCDS MFC treatment:
I have not done as much research on the TM surgery and where it is performed. I know they do it at Stanford but you should do your own deeper research on this topic.
I was ecstatic with the team at UCLA but I heard great things about these other teams as well. Please do your own research, meet with the surgeons you narrow down to and make the best decision for you. Note, that this is a slow process because as you can imagine, these are very busy doctors and there is a waiting line to first see them, then to schedule the surgery

In 2007 (or 2008 I don't remember exactly) I had a pretty bad concussion playing soccer where I lost consciousness for minutes, as by the time I woke up the ambulance was already there. I went to Stanford's ER where they did a CAT scan and dismiss me right away. In the following months, I experience some isolated episodes of vertigo, which went away over time by doing the Epley maneuver as documented in this video.
After that, I went back to a normal very active life playing soccer, tennis, and skiing without problems.
We don't know for sure, but this could be the seed that started the development of my SCDS
In 2009, I went to an AC/DC concert that was really, really loud and fir the first (and only) time in my life, I experience vertigo triggered by the loud sounds coming out of the music speakers. I had ringing in my ears for a week. I am not sure this was related to SCDS slowing developing in my inner ear but it is probably worth mentioning it.
In February 2017 I had an episode where I really lost my temper and raised my voice. The reason I mentioned this is that after that happened, I felt pressure inside my head for maybe an hour of so as I was having a hard time calming down. Again, it is hard to tell for sure, by my SCDS symptoms started around the same time.
After taking one year off work, in May 2017 I started a new job and in the couple of months leading to it, I started noticing a pulsating whooshing sounds inside my left ear that would get lauder if I bended forward, or grinned my teeth. Initially, I did not think too much of it but it got laud enough that I wanted to see my family doctor about it.
The doctor ordered a hearing test and then saw me. The test showed a slight loss of hearing in both ears but a little more prominent in the left ear, loss compatible with my age and exposure to noise both on the job but especially as a life long amateur musicians.
The doctor say that I had pulsatile tinnitus, like around 40% of aging adults and that I would have to just deal with it because there is no cure for it.
After few weeks the noises got louder. I started to notice that beside hearing my heart beating in the form of a pulsating whooshing sound, I started to hear my own voice loud and distorted in the left ear that made it difficult to speak and communicate with others. When I told my family doctor, he immediately scheduled a visit with an ENT specialist to go deeper.
As soon as I told the ENT specialist that I had these symptoms in my inner ear and that they got worse pretty quickly, he immediately ordered a fine grained CAT scan. They want to see if there is something growing inside your head who is creating pressure of sort. It is important that the CAT scan is 0.24 millimeter to detect SCDS.
When the results were back I was initially relieved as it was negative for all the bad things one may fears, e.g. cancer, but there was a sentence in there along the lines of "compatible with SCDS".
I asked the ENT and he told me that it is a rare syndrome and that I was lucky because the doctor who discovered SCDS at john Hopkins now works at Stanford and he was going to refer me to Dr. Blevins in his team who would look at me and assess my options including surgery.
While I was of course a little concerned about all this, I was happy help was around the corner.

Unfortunately the soonest Dr. Blevins could see me was 5 months out in September. I started to panic and went online to do more research. This is when is gets really scary as you learn about other patients that are effected by horrific symptoms and the mind wonders. How do I deal with this? What if it gets worse? What do I do??
This is when I ran into the Facebook support group ran by Pamela Gilbert where I found a lot of helpful information and around 2000 members who are fighting this syndrome and help each other.
This was definitely the lowest point of the journey where I did not know enough about the syndrome, what to do about it and how to manage my symptoms. In the meantime I have a brand new pretty high pressure job where I need to establish myself and get traction.
I am a super positive, very active and energetic person and I thought I would be able to deal with it like anything else that life has thrown at me. But I was wrong.
Despite all my best efforts to stay positive, try to think about other patients with worst symptoms or people in terminally ill conditions, I just could not help going back thinking about my own situation and getting more and more negative, dare to say... depressed.
Initially I only told my wife and a couple of close friends. Interestingly nobody could really tell, but my 80 years old mom who was here visiting from Italy knew something was off. She saw it in my eyes. She kept telling me "what's wrong with you Vittorio, your eyes are not smiling"
After doing my research on SCDS surgery, I landed on UCLA because of their experience, innovative approach to the surgery and proximity (they are a quick 1 hour flight away from where I live). I contacted Dr. Yang over email who to my surprise replied within minutes. We scheduled a phone consultation to go over my CAT scan and discuss options. He confirmed the diagnosis and we agreed that I should fly and go meet with him and Dr. Gopen (the ENT Surgeon who works with him to cure SCDS at UCLA). He said this surgery surgery has a very high success rate and it was an option for me.
Well, great news but... here is the kicker... it is still a small brain surgery and altho they don't really do much with the brain other than lifting it, it is a pretty scary proposition at first.
I scheduled a visit
At this point, I am not sleeping much at all. At night symptoms are the worst because that's all you hear, and right when you think you are falling asleep, the heart beat wakens you up and panic kicks in. You have to walk, go outside, gets some fresh air...
I am a pretty avid espresso drinker. I tried quit drinking coffee to see if that would help. It did not. I quit cold turkey and I went through withdrawals only to realize that not having coffee in the morning threw my body rhythms off even further. I tried Chamomille and decaf tea without getting much relief.
While the call with Dr. Yang gave m some comfort, at this point I can't take the elevator, the idea of being closed in a small environment, especially with other people drives me crazy. Forget about getting on a place for business travel. Amazingly I cant still function relatively well at work and I am getting traction with the new job, but it requires a tremendous amount of energy.
I cannot even stand having my wedding ring on... I need something to deal with all this and manage potential panic attacks. So I cal my doctor who prescribed Lorazepam 0.5, an anti-depressant.
Of course, even if I am feeling like crap, the way my mind works pushes me to consider the long term consequences of my actions, so I research the drug and learn about the side effects of it. I am afraid of long term addiction even thou the doctor says that people don't get addicted from short term use.
Anyway, I wrap two pills and put them in my wallet for emergencies and decide not to take the drug on a regular basis. Again, everybody should do what's right for them. These type of drugs help many, many people deal with all sorts of situation. I just did not want to do it.
I figured that if I could sleep a little better, I could get to a better place. So I started to take Advil PM or Benadryl and Melatonin. Advil helped a little, but you know where this is going already, I did some research and realized that even these drugs have long term impact on your cognitive skills. I can't afford that. My brain is the bread maker, I cannot risk it.
Enters Tennis and Meditation

I credit the progress I made in managing my symptoms to playing tennis and meditation.
In September 2017, I flew down to Los Angeles to the Ronald Regan UCLA medical Center to meet with Dr. Gopen and Dr. Yang to discuss my options in person. The bottom line from our discussions was
Dr, Yang explained how they use advanced imaging, computer graphics to simulate the surgery ahed of time virtual reality to identify where to open a small hole in the skull to reach the dehiscence in the inner hear.
Then Dr. Gopen explained to me how he goes in there and resurfaces the superior canal with bone wax, a inert material that has been successfully used in surgery application since world war two. He also explain that he does not plug the hole, and therefore the upper canal to preserve the balance organ. I liked that.
I am a geek and sucker for great technology, but I liked the whole approach and the fact that this team is one of the most experienced ones in the world along side John Hopkins and Boston Eye and Ear Hospital.
It seemed like a no brainer (no pun intended) decision to make. I was definitely leaning towards getting surgery
In the mean time my appointment with Dr. Blevins at Standford is up. I would be great to get a second opinion. Dr. Blevins did a thorough evaluation of me and my CAT scan and confirmed the diagnosis. He told me that at Stanford they perform TM surgery where they drill a hole in the temporal bone on the side of the ear, reach the superior canal, cut it and plug it completely. This mean you lose the use of the balance organ on that side, and over time the brain learn to rely on the other ear. While this approach has proven to be viable, especially with patients with balance problems, I did not think it was the right things for me, as I did not have balance problems and I want to live a very active life.
Dr. Blevins also scheduled a Vemp test that again confirmed the diagnosis.
At this point I have done my research, met with the team at UCLA and got a second opinion from Stanford. Altho I am finally managing my Symptoms much better, I still get tired easily and I am still experiencing brain fog. Again, people can't tell, but I know. It is time to get it done, so I schedule the surgery for November.
Later that months, I learned that my company was getting acquired and being part of the team working on the due diligence, I decided to post-pone the surgery to January 25th 2018.
In all this, I consider myself a very, very lucky person. Here are the main reason why

The way at team at UCLA organizes the Surgery (as of January 2018) works like this:
Here is the strategy that I used to prepare myself for surgery:
I was definitely ready for surgery
I drove down to Los Angeles on Sunday as I had an errand I had to run before surgery in the area and to visit my daughter at UCI (University of California Irvine). I rented a condo via AirBnb less than a mile from UCLA, which was a good call as it was convenient, cheap and give you a more home-like feeling than staying in an hotel room.
Here is when I started to document my experience with daily videos, which I believe is the most valuable part of this website. While there are many SCDS user stories on YouTube, I could not find a detailed, step-by-step chronicle of what it means to get SCDS surgery, in my case MFC (Middle Fosse Craniotomy) with the Keyhole technique. So here it goes...

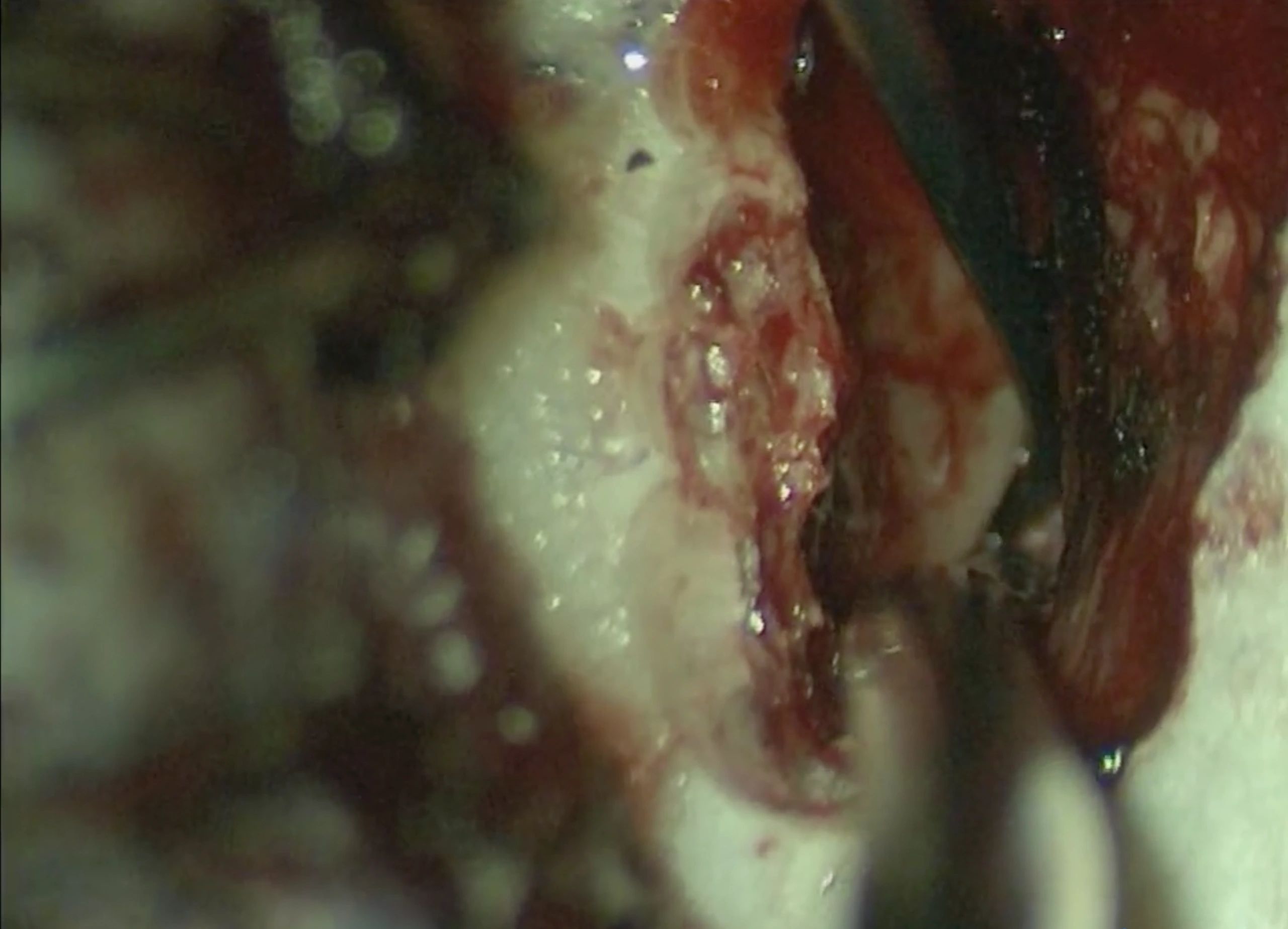
There is the little hole (dehiscence), in the left Superior Upper Canal if the inner ear. Damn you hole!!

Here is the scar a day after Surgery
The super small "keyhole" opening in the skull to reach the inner ear
The super small "keyhole" opening in the skull to reach the inner ear
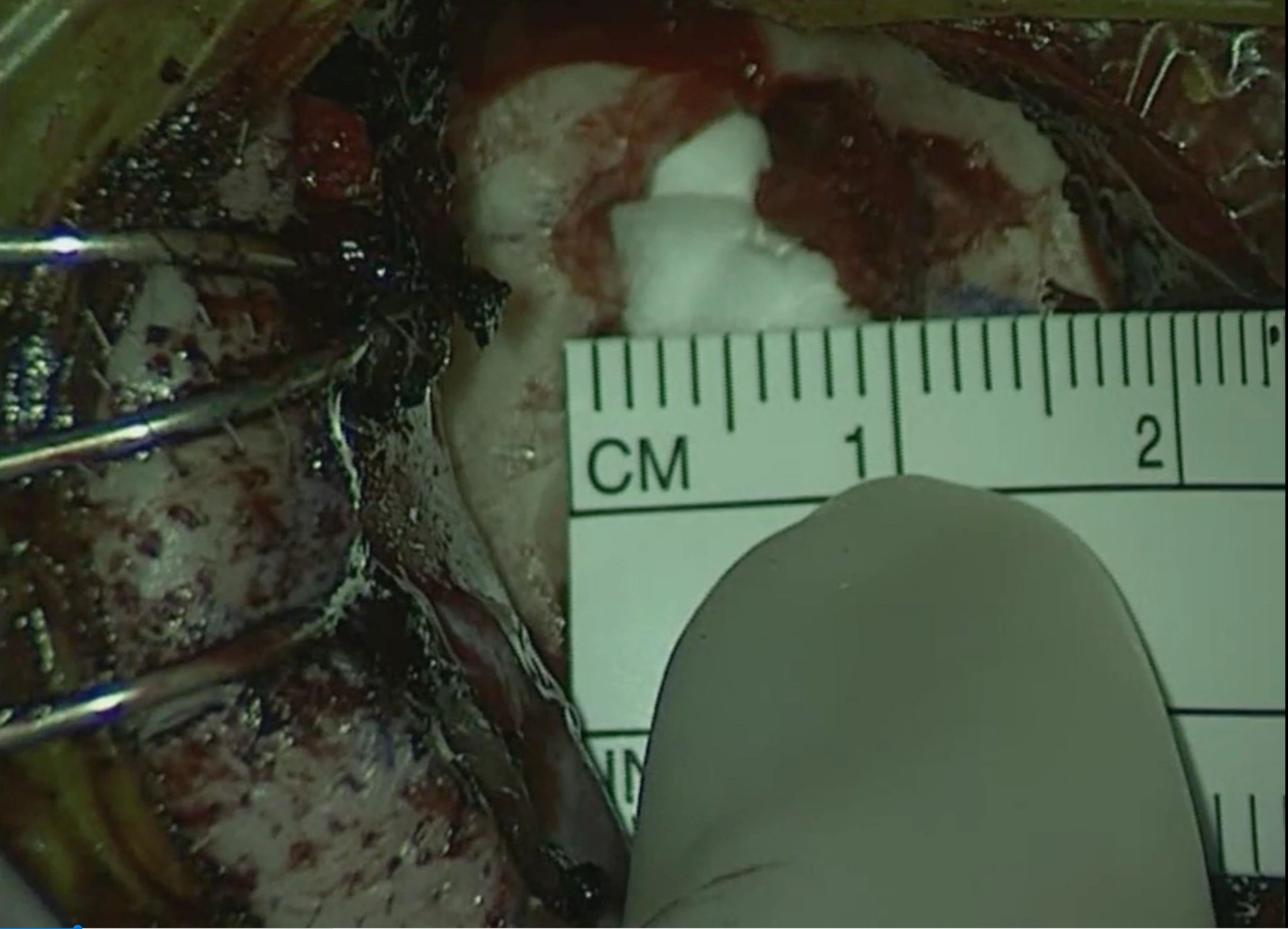
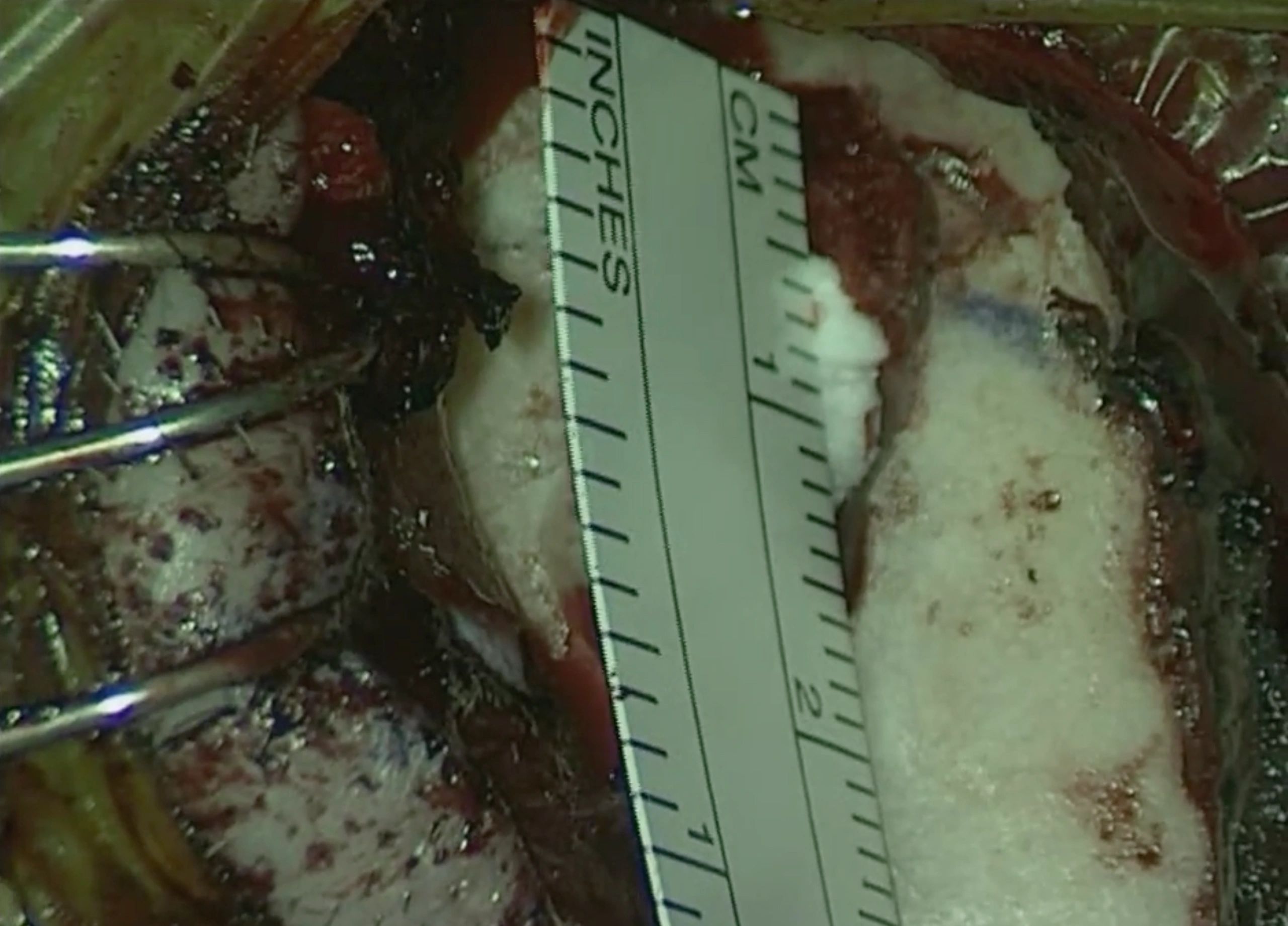
Here is the hole in the inner hear to the right of the bone and to the left of the brain base
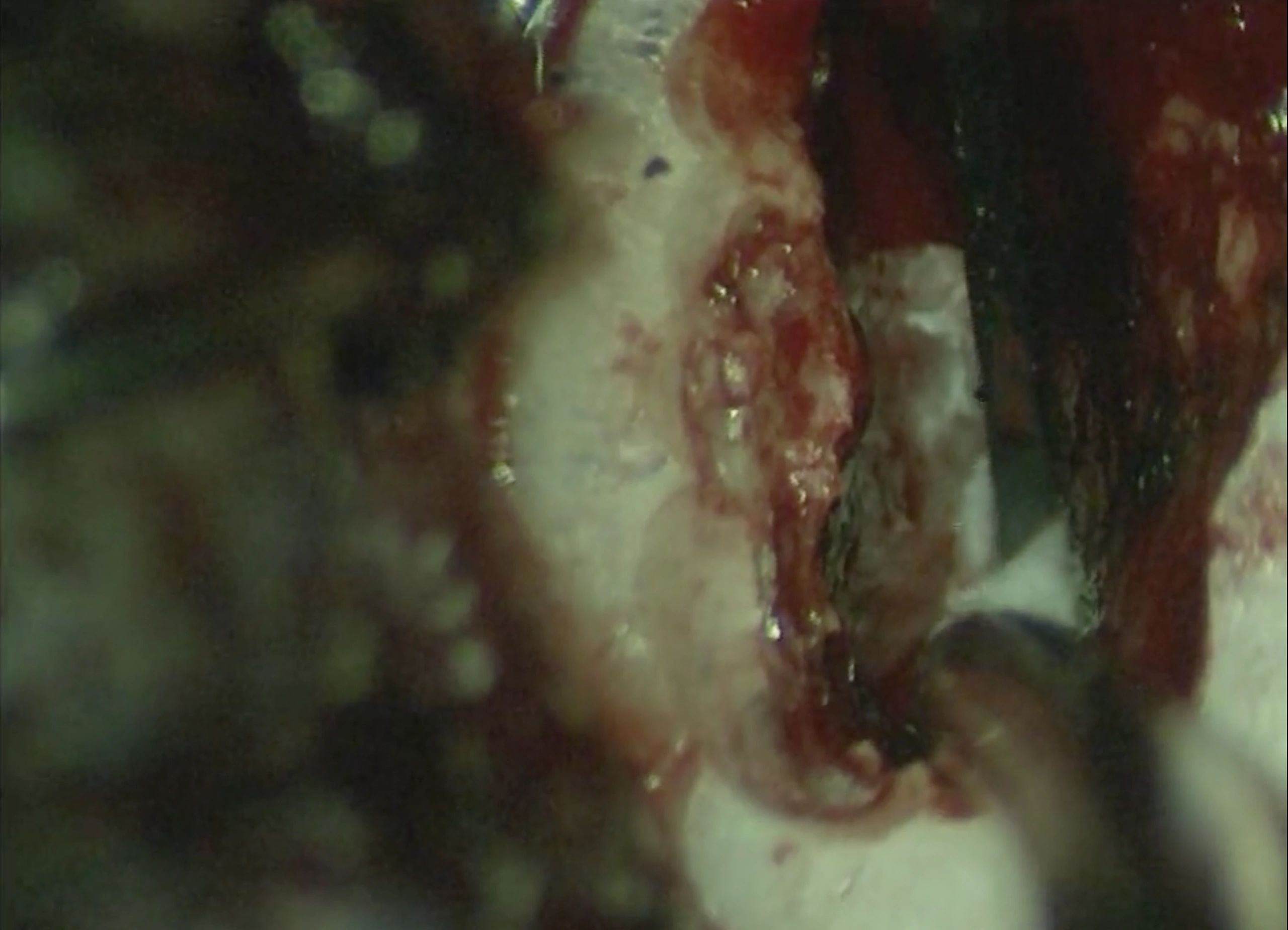
Dr. Gopen resurfacing the dehiscence (hole) with bone wax